
Valproate, in its many forms and with different names (valproate, valproic acid, divalproex, Depakote, Depacon, Depakene), is a drug that has been used to treat various disease states since the 1970s at a minimum. From bipolar disorder, to migraines and seizures, valproate has found itself in the arsenal of many clinicians. However, it does come with one side effect that is rarely consequential, but when it does appear, it blurs the lines of what is really going on with the patient. Valproate can cause hyperammonemia, even in the absence of hepatic injury!

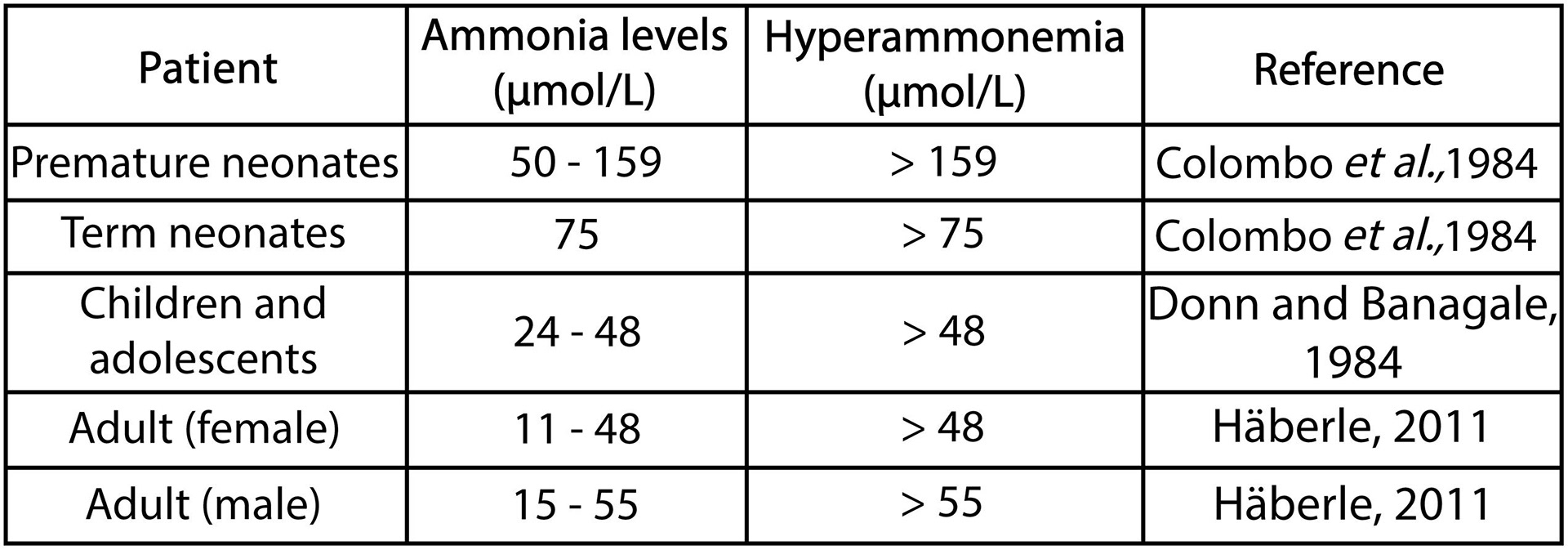
BACKGROUND: As a refresher, hyperammonemia, or elevated levels of ammonia, can cause encephalopathy with symptoms that range from confusion to a coma-like state, and can even cause seizures and cerebral edema if left untreated. If you’re like me, the default answer to the cause of elevated ammonia is some sort of liver abnormality. Thus, we usually see some degree of LFT abnormalities if an elevated ammonia is present.
PATHOPHYSIOLOGY: Except valproate can cause hyperammonemia WITHOUT any elevation/abnormalities to LFTs. Why is that? Well, Valproate and its derivatives inhibit the production of a molecule N-acetyl glutamate (NAG), which is essential for the urea cycle. In fact, this is the rate limiting step of the urea cycle! Without NAG, ammonia remains ammonia and does not become urea. Thus, patients on valproate therapy are predisposed to hyperammonemia even if their LFTs are completely normal.
PREVALENCE: In one study of 347 patients on valproate therapy, 36% of these patients had an ammonia level above this institution’s definition of normal. Of the patients with hyperammonemia, 43% were symptomatic. I think this goes to show that hyperammonemia among patients on valproate therapy is actually more common than clinicians have come to believe. Additionally, with many of these patients being acutely symptomatic, it’s imperative to recognize this as something that needs evaluated on patients taking valproate presenting with any sort of altered mental status.
TREATMENT: The most successful treatment for valproate-induced hyperammonemia is discontinuation of the drug. Lactulose and therapy with L-carnitine were also used with moderate success.

CARNITINE: Valproate is known to deplete stores of carnitine. Valproate both binds to and inhibits production of carnitine, meanwhile, elimination of valproate is also dependent on carnitine! This creates a positive feedback loop that results in even more valproate in the system and even less carnitine. This is why with valproate-induced hepatotoxicity and even hyperammonemia, supplementation with IV L-carnitine may prove beneficial to prevent further damage to the liver and help eliminate valproate from the body.
SUMMARY: All things considered, valproate is a commonly used drug in society today. However, I feel that this particular side effect flies under the radar in education for providers and pharmacists. With proper awareness guiding our decision-making, I’d encourage any provider who receives an altered patient that takes valproate to add an ammonia level to the labwork. The results you find may surprise you.
SOURCES:
1. Baddour, Elisa, et al. “Valproic Acid–Induced Hyperammonemia: Incidence, Clinical Significance, and Treatment Management.” Mental Health Clinician, vol. 8, no. 2, Mar. 2018, pp. 73–77, https://doi.org/10.9740/mhc.2018.03.073.
2. Malaguarnera, Mariano. “Effects of L-Carnitine in Patients with Hepatic Encephalopathy.” World Journal of Gastroenterology, vol. 11, no. 45, 2005, p. 7197, https://doi.org/10.3748/wjg.v11.i45.7197. Accessed 30 Nov. 2021.
3. Limketkai, Berkeley N, and Stephen D Zucker. “Hyperammonemic Encephalopathy Caused by Carnitine Deficiency.” Journal of General Internal Medicine, vol. 23, no. 2, 13 Dec. 2007, pp. 210–213, https://doi.org/10.1007/s11606-007-0473-0. Accessed 1 Apr. 2024.
4. Lheureux, Philippe ER, et al. Critical Care, vol. 9, no. 5, 2005, p. 431, https://doi.org/10.1186/cc3742.