
In the emergency department or other acute care settings, muscle relaxants are relatively commonplace for patients with relevant musculoskeletal pain. However, is there a clear cut choice for when to use a specific agent, other than “yeah I’m feeling Valium today”? Let’s explore!

Diazepam (Valium) – Benzodiazepine that binds to the GABA-A receptor, which increases the length of time that neuronal chloride channels are open. This produces a hyperpolarized state such that the neuron cannot transmit as many signals (of pain/spasticity in this case). Diazepam is active at GABA receptors in the brain AND the spinal cord, and its spinal cord neuron inhibition is the reason for its potency as a muscle relaxer. Diazepam is not appropriate for patients with liver dysfunction or elderly patients since the reduced clearance of medication makes its pharmacokinetics more unpredictable. However, short-term treatment with diazepam does not need adjustment for renal impairment, so that's a plus.

Cyclobenzaprine (Flexeril) – A muscle relaxer very closely related to tricyclic antidepressants, cyclobenzaprine acts on central alpha and gamma motor neurons in the brain stem to reduce tonic somatic motor activity. It also has 5-HT2 antagonistic properties. Bearing in mind that antipsychotic medications agonize 5-HT2, it’s easy to associate antagonism of this receptors with antispasmodic properties due to the dyskinetic effects produced by antipsychotics. Being in the tricyclic family, cyclobenzaprine is not appropriate for older patients or patients with liver dysfunction. Use in patients with renal dysfunction is a gray area but the limited data we have suggests that it is safe.

Methocarbamol (Robaxin) – Centrally acting muscle relaxant that is poorly understood from a mechanism standpoint. It is theorized to produce anticholinergic CNS depression in the midbrain, which produces overall sedative effects that extend to the muscles. It has no synaptic properties at the muscles themselves. Being anticholinergic, this is generally not appropriate for older patients. There is also limited data on patients with renal/hepatic insufficiencies, so proceed with caution in these populations.
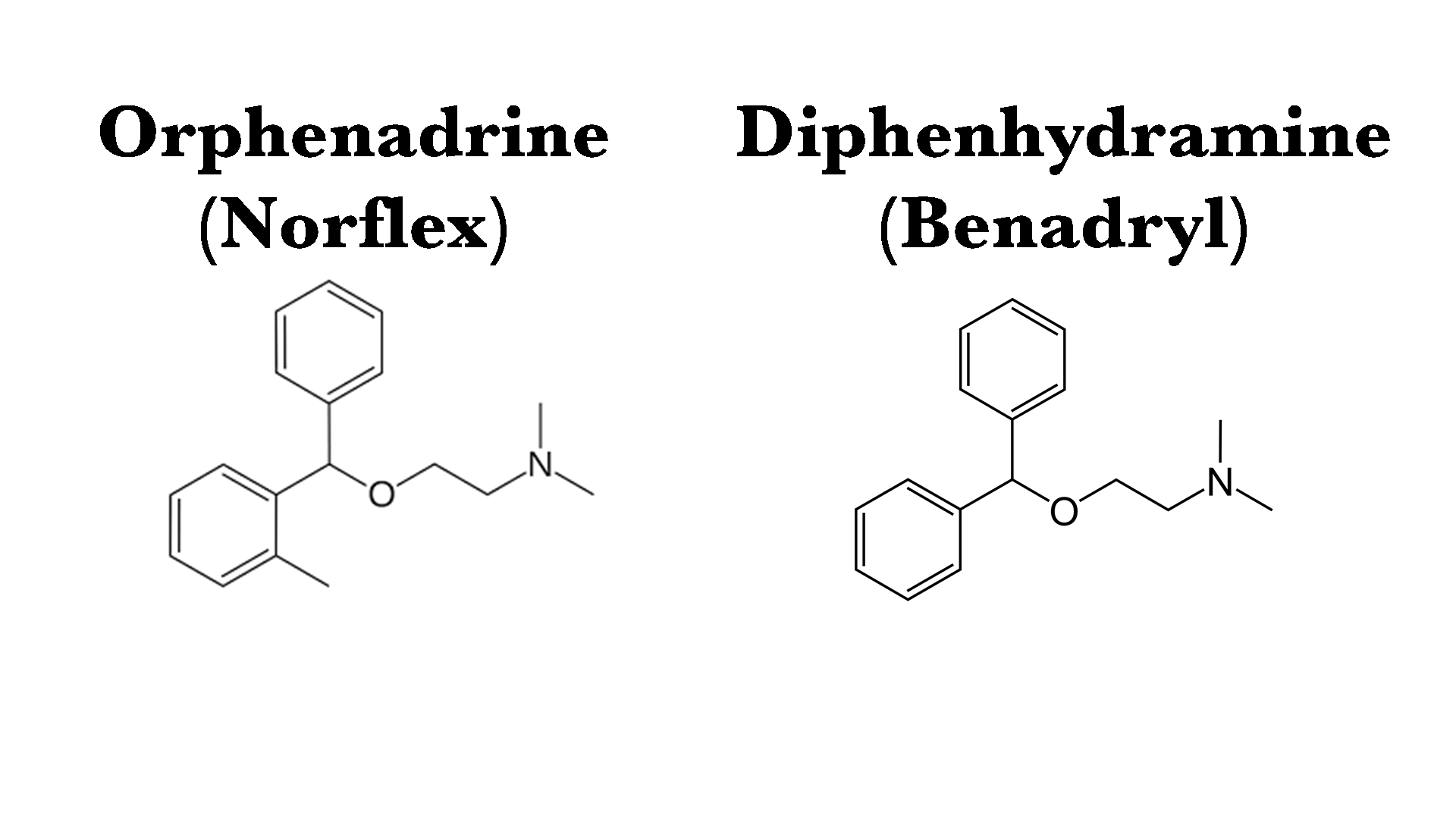
Orphenadrine (Norflex) – If we are explained Norflex to patients the way I’m about to explain it to you, they’re probably going to ask for something else. Orphenadrine is a centrally acting antihistamine, anticholinergic, and NMDA receptor antagonist and it is literally methylated diphenhydramine. Yes, add a methyl group to a molecule of Benadryl and you get Norflex. Why this mechanism reduces musculoskeletal pain is poorly understood, though it’s proposed that the central CNS depression reduces central perception of pain. Norflex: you can’t be in pain if you’re not awake to perceive it. As you can imagine, this medication is not appropriate for older adults. HOWEVER, there are no dosage adjustments provided in the labeling for either renal or hepatic impairment, so have at it!

Metaxalone (Skelaxin) – So you’re probably not ready to hear this, but metaxalone is an oxazolidinone. If you are triggered by this word since you’ve heard it before, I’ll help you out. The antibiotic Linezolid is also an oxazolidinone. Once again, Metaxalone is a general CNS depressant with a poorly understood mechanism that is thought to reduce central perception of musculoskeletal pain. With this mechanism, it also lands itself on the Beers criteria and should generally be avoided in elderly patients as well as patients with renal/hepatic impairment.

Baclofen (Lioresal) – Finally a Beers-friendly (as in Beers-criteria, not beers-alcohol) muscle relaxant! Baclofen has a mechanism that should be relatively clear if I call it by its other name: beta-4-chlorophenyl-GABA. Yes, it’s a beta GABA receptor agonist! It also has an affinity for voltage gated calcium channels, causing hyperpolorization and acts mostly at the spinal cord level to reduce monosynaptic and polysynaptic reflexes. Through spinal cord GABA agonism and reduced neuronal reflexes, the patient perceives less musculoskeletal pain. Baclofen should be used in short courses (3-5 days) at the maximum for this purpose to avoid withdrawal. There are no dose adjustments necessary for hepatic impairment, but for patients with renal insufficiency the dose should be reduced, or if the CrCl is < 30mL/min use should be avoided.
Tizanidine (Zanaflex) – These would not be the “Xans” people want, but they’re the “Zans” they should get. Tizanidine/Zanaflex is an alpha2 receptor agonist, which reduces excitatory neurotransmitter release like glutamate and aspartate. I like to think of the mechanism like this: if your adrenergic receptors are being occupied by Tizanidine, the body needs to down-regulate its production of adrenergic molecules like epi/norepinephrine and excitatory neurotransmitters that come with them. This reduces the passage of pain signals through the neurons of the spine to reduce perception of pain. Once again, this is a preferred, Beers-friendly medication. It will require dose adjustment for renal dysfunction and should be avoided in patients with hepatic impairment.
Carisoprodol (Soma) - We’re back to medications on the Beers list. This is another medication that is poorly understood from a mechanism standpoint, but is generally thought to be a centrally acting overall CNS depressant. It is a controlled substance that should largely be avoided in older adults and patients with either renal or hepatic impairment. There’s better and easier options out there, so I don’t prefer Soma.
To summarize muscle relaxants in a nutshell:
-Elderly patients: Baclofen or Tizanidine >>> everything else
-Renal impairment: Diazepam > Orphenadrine, Methocarbamol, or Tizanidine > everything else
-Hepatic impairment: Baclofen or Orphenadrine > Methocarbamol > everything else